In September 1991, the 2000 persons received an invitation to participate along with a questionnaire about general demographic information and lifestyle, signed by their general practitioner. All who agreed to participate received an extensive supplementary baseline questionnaire with detailed questions that evaluated the participant’s health, lifestyle, psychosocial status, and psychosocial life events. Participants were informed by their general practitioner about which intervention they would be offered.
Randomization
Participants were randomly assigned to 1 of 3 groups by proportional, stratified randomization based on the general practitioner with whom they were registered, their sex, age, cohabitation status, and body mass index (BMI). All 3 groups received questionnaires. Health screenings were offered to 2 of the groups and follow-up health discussions with the general practitioner were offered to participants in only 1 of the 2 intervention groups. An employee of Aarhus County who was not otherwise involved in the study carried out the randomization.
Health screenings
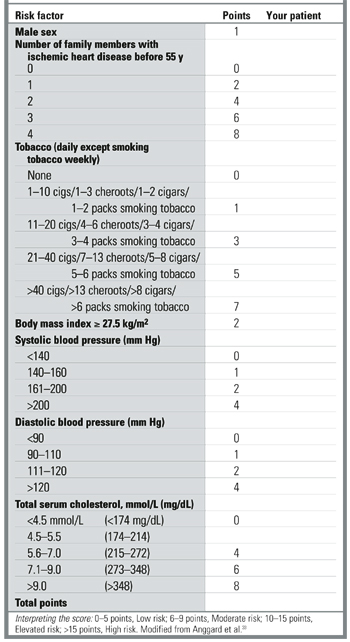
Participants were given a multiphasic, broad-spectrum screening. This included a calculation of cardiovascular risk score (CRS), giving an estimate of the risk of premature cardiovascular disease for each individual. Figure 1 shows the calculation of CRS based on sex, familial inheritance (number of family members with ischemic heart disease before age 55), tobacco use, blood pressure, serum cholesterol (total), and BMI33 and the subsequent division into risk groups. Baseline health screenings were performed by 3 laboratory assistants between December 1991 and June 1992 and took place in the town of Ebeltoft, in the central clinic which 5 of the general practitioners shared. A few weeks after the health screening, all those tested received personal written feedback from their general practitioners. Where values fell outside the normal range, the feedback included advice relating primarily to lifestyle changes. All participants who had been advised that they had an elevated or high CRS were encouraged to see their general practitioner, regardless of their randomization group. All tested participants also received pamphlets on leading a healthy lifestyle from the Danish Heart Foundation.
FIGURE 1
Calculation of cardiovascular risk score
Health discussions
A 45-minute consultation with their own general practitioner was offered to participants from the health screening plus discussion group. Prior to the consultation, the participants completed a short questionnaire about suitable topics for discussion. At the end of the consultation, general practitioners invited participants to set a maximum of 3 health-related lifestyle goals for the following year. In cooperation with the participant, general practitioners then recorded these goals in a separate questionnaire.
Follow-up
Follow-up took place 1 and 5 years after the baseline intervention. Participants received follow-up questionnaires and were offered health screenings and health discussions according to their group of randomization. Participants in the health screening plus discussion group were offered annual consultations. The control group was promised a health screening and a health discussion at the end of the study period. Other details of the design are outlined elsewhere.23
Data analysis and statistics
SPSS version 9.0 for Windows was used to analyze results. Double data entry was used for the laboratory tests. Differences between groups were evaluated by 2- test for categorical data, by t-test for means, and by nonparametric testing for nonparametric data. Ninety-five percent confidence intervals (95% CI) were applied to relative risk (RR) values. Information was used from the baseline questionnaires to identify baseline risk groups among all those randomized. At the 5-year follow-up, randomized groups were compared according to the intention-to-treat rule (ie, regardless of their compliance with the intervention program).
Results
Participation at baseline and follow-up
Seventy-five percent (1507) of the 2000 persons invited to participate agreed to take part in the study. The percentage was higher among women (80.0%) than among men (71.0%).
Table 1shows the distribution of sociodemographic and cardiovascular risk factors at baseline among the randomized groups. No significant differences between groups were found. General practitioners advised 11.4% (103 persons) of the 905 tested in the intervention groups that they had an elevated or high CRS (≥10) at baseline. Of these, 52 belonged to the health screening group and 51 to the health screening plus discussion group. Prior to the test almost all participants were unaware of any existing cardiovascular disease.
Of the 443 persons in the health screening plus discussion group who accepted the offer of a consultation, 307 (69.3%) (95% CI, 64.8%–73.6%) decided to change their lifestyle in 1 or more respects. The number was significantly higher among those who had been advised of an elevated cardiovascular risk and who accepted the offer of a health discussion: 46 of 51 (90.2%) (95% CI, 78.6%–96.7%). In decreasing frequency, the goals set related to weight (63%) (95% CI, 47.5%–76.8%), diet (50.0%) (95% CI, 34.9%–65.1%), physical activity (50.0%) (95% CI, 34.9%–65.1%), smoking (43.5%) (95% CI 28.9%–58.9%), alcohol use (17.4%) (95% CI 7.8%–31.4%), and work (13.0%) (95% CI, 4.9%–26.3%). Emotional well-being, drug treatment, and other subjects (in each case by 2 different participants) were also discussed.