Recent studies on fibromyalgia and pain
Fibromyalgia (FM) may be considered the prototypical central pain disorder, in which the pain originates or is maintained in part in the central nervous system. Although new diagnostic criteria are being validated for this disorder, FM classically has been diagnosed by the detection of 11 of 18 tender points and the presence of chronic widespread pain for 3 months or longer.12
FM is a common disorder found to affect between 2% and 4% of the US population.13 It was one of the first disorders shown to have central factors predominant in the pathology, and as a result it has been the focus of numerous studies. Irritable bowel syndrome and chronic fatigue syndrome, often comorbid with FM, are also commonly studied. Until recently, these disorders have largely been considered “wastebasket” terms to categorize the complaints of patients with unexplained symptoms, because there were no objective signs to support their complaints. However with the advent of new imaging techniques to look into the brain and the central nervous system, researchers are finding very real physiological differences. For example, one study using sensory testing with thermal, mechanical, and electrical stimuli showed a correlation between FM patients’ subjective reports of pain and significantly altered cold and heat thresholds when compared with controls.14 Based on such studies it appears that patients with FM perceive stimuli as noxious at lower levels than healthy, pain-free controls.
Recent studies of FM have incorporated the use of functional magnetic resonance imaging (fMRI) to look at brain activations in response to painful stimuli. A study that included patients with FM and others with chronic low-back pain used fMRI to visualize the participants’ response to equal amounts of thumbnail pressure. In the FM and groups, 5 areas of neuronal activation within the cortex related to pain were detected, compared with only one activation in controls.15 Another study to evaluate the pattern of cerebral activation in FM patients found that in response to similar thumbnail pressures there were 13 regions of greater activation in the FM group compared with one region in the healthy control group.16 Additionally, mild pressure resulted in subjective pain reports and cerebral responses in the FM group that were similar to responses produced by twice the pressure applied in controls.
Another important area of research in pain processing looks at gray matter in the brain using voxel-based morphometry. A study of patients with FM found significantly less volume of gray matter and an age-associated decrease in gray matter that was 3.3 times greater than healthy controls.17
Using MRI to look at gray matter volume in patients with chronic musculoskeletal pain, significant differences in gray matter volume were found in osteoarthritis patients prior to hip arthroplasty compared with healthy controls. Specifically, areas of the thalamus, understood to play a role in central pain processing, showed decreased gray matter volume in the osteoarthritis group. Significantly, a comparison of gray matter volume 9 months after surgery showed that the levels of reduced thalamic gray matter volume in osteoarthritis patients “reversed” to levels similar to the those of the healthy control group.18
Although the mechanism that drives the loss or degradation of brain tissue in patients with chronic pain remains to be determined, one theory is that pain is associated with certain areas of the brain becoming hyperactive. Imaging studies using fMRI show that a constellation of regions typically are activated in pain processing, including the insula,
cingulate, primary somatosensory and secondary somatosensory cortices, amygdala, and thalamus [Figure 2].19 These regions have been shown to be more active in chronic pain states when patients respond to stimuli such as painful pressure or heat. Indeed, these regions have shown overamplification or augmentation of neural activity.
| FIGURE 2: Neuroanatomy of pain processing. Main brain regions that activate during a painful experience are highlighted as bilaterally active but with more dominant activation on the contralateral hemisphere (red). |
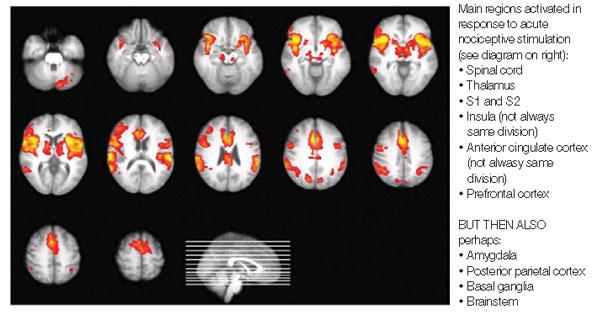
| Source: Tracey I. Br J Anaesth. 2008;101:32-39. |
Since overstimulation of nerve cells can trigger a toxic release of glutamate into surrounding tissues of the brain, this may cause nerve cells to die, ultimately reducing the amount of gray matter visualized in the brains of patients with chronic pain. In addition, some studies of FM have shown elevated levels of glutamate, an excitatory neurotransmitter that is known to cause excitotoxicity.20
Another significant consequence of long-term pain appears to be alterations in the normal connectivity of the brain, including the “default mode network” (DMN) which is noted to be important during the resting state. Recent studies of chronic pain suggest alterations in key DMN regions that may be related to the chronic pain state and existing comorbidities.21