"My mother-in-law did not allow me to go to the hospital," she replied, and stars started twinkling in her eyes.
She had become pregnant some 9 months ago, and she was very happy. She dreamed of a fairy baby all the time. She is a maid at our house and comes daily from the nearby urban slum to do the household chores. Since she got pregnant, my wife became her "consultant obstetrician."

By Dr. Ghulam Mustafa
She was worried when she started "vomiting" when she smelled various smells, especially in the kitchen. My wife advised her to go to the nearby tertiary care hospital for her first antenatal visit. A few days later when my wife asked her if she had gone to the hospital, she replied, "nay." "Why?" asked my wife. The answer was, "My mother-in-law did not allow me." The time went on, and she was filled up with baby and joy. Eventually the day came when it became difficult for her to wash clothes and stand for long. She requested "maternity leave" and was given such.
But when she came back, she came without a baby. "Where is your baby?" my wife asked. "He died during delivery," was the reply. "The baby got stuck on his way out. The Dai (unskilled traditional birth attendant) tried to pull [the baby out], but she failed," she said. "Why you didn’t go to the hospital?" we asked. The reply was, "My mother-in-law did not allow me to go to the hospital."
The million-dollar question was why this mother-in-law did not allow her to go to the hospital. When I probed, it surfaced that such elder women were convinced that the government facilities did not cater to the poor patients with care. This belief led them not to follow the health advice that was being given by the scientific community.
We pondered over it. The International Community Access to Child Health (I-CATCH) project came exactly at the right time, and we started the Helping Hands project to motivate people, especially women. The community health worker (CHW) was selected from the same community and trained with multiple health messages. The messages included antenatal care, need for delivery at a health care facility, tetanus shots for mothers, exclusive breastfeeding for the first 6 months, vaccination for the babies, hand hygiene, iodized salt, hepatitis B vaccination for all, child and especially female education. The CHW started working door to door without leaving out any house. They would chat with mothers, dispel their fears, and motivate people to use proper health practices.
The key to success was the door-to-door visits of the CHWs and their persistence. Usually each house was visited once every month. There was minimal response for the first 10 visits, and we were quite hopeless for the progress. But then there was a response, and that response was so marvelous that it would not be wrong to call it miraculous.
A woman came to see me and told me that she has been isolated and abandoned by the whole family. She said, "They have separated me. I have a separate room, separate toilet, and separate utensils, and no one comes near me. My husband does not touch or kiss me any more or even sit with me." I asked why they were doing this. "They say I have hepatitis C."
I told her that the first thing she needed to do was to get a reliable report of her hepatitis C status and that hepatitis C was not spread by eating or living together. "But who is going to tell all this to my family?" she asked. I promised that we would do it.
Our CHWs did sensitize not only her family, but the whole community. Later the woman was found to be hepatitis C-negative by enzyme-linked immunosorbent assay (ELISA). But the sensitization worked to the extent that almost the whole community got themselves vaccinated against hepatitis B.
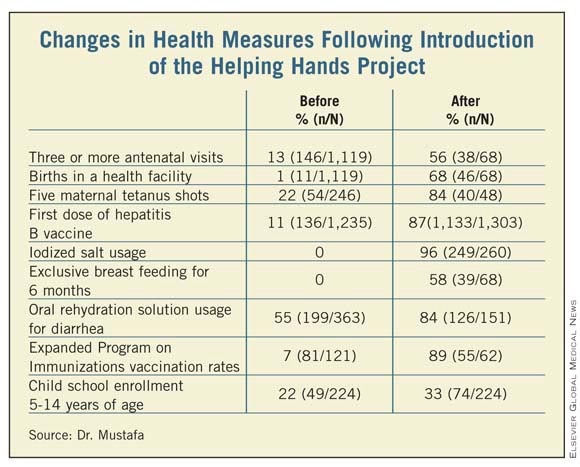
Indeed, after 18 visits there were changes in the percentages of women receiving antenatal care, deliveries at health care facilities, tetanus shots for mothers, exclusive breastfeeding for the first 6 months, vaccinations for babies, hand hygiene, use of iodized salt, hepatitis B vaccinations for all, etc.
The phenomenon has inspired the people around us, and we are planning it on a large scale at multiple sites. The people are ready and have committed to adopt the model in their neighborhood when we are ready with our infrastructure of software to tackle such a large, variable, and ever-changing task.