Colin W. Howden, MD Professor of Medicine, Division of Gastroenterology, Northwestern University, Feinberg School of Medicine, Chicago, IL William D. Chey, MD Associate Professor, Division of Gastroenterology, Director of the GI Physiology Laboratory, University of Michigan Health System, Ann Arbor, MI *This special section of The Journal of Family Practice is provided by an unrestricted grant fromTAPPharmaceutical Products, Inc. The authors received a stipend for this work. Dr. Howden reports that he serves on the speakers bureaus for Merck &Co., Inc., Novartis, TAP, and Wyeth, and he has been a consultant to Novartis, Prometheus Laboratories, Inc., Takeda Pharmaceuticals North America, TAP, and Wyeth. Dr. Chey reports that he has received grants and/or serves on speakers bureaus for AstraZeneca, Janssen, and TAP.
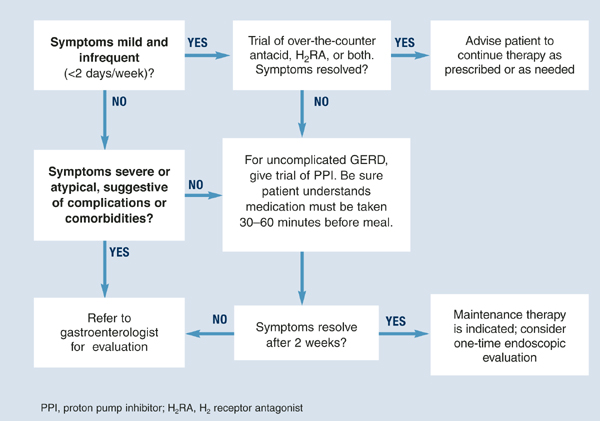
Diagnosis is usually based on typical symptoms—heartburn or regurgitation—in the clinical history. (The Figure shows a treatment algorithm for both severe and mild symptoms.)
A 2-week trial of treatment with a proton pump inhibitor (PPI) provides the quickest and most cost-effective confirmation of diagnosis and is recommended for the patient whose history suggests uncomplicated GERD. A positive response to PPI treatment in a patient with symptoms suggestive of GERD is at least as sensitive and specific as 24-hour intraesophageal pH monitoring, which is still often considered the “gold standard” for the diagnosis of GERD. Furthermore, complete lack of improvement in response to PPI treatment is highly predictive that the patient does not have GERD and indicates the need for further evaluation and a possible revision of diagnosis.11,12
H2 receptor antagonists (H2RAs) have also been investigated in empirical trials for usefulness in diagnosing GERD. H2RAs are less effective than PPIs.13,14
FIGUREMedical management of suspected GERD
Endoscopy
No data support routine endoscopy for patients with the recent onset of uncomplicated heartburn who respond to medical therapy. Endoscopy is recommended, however, for patients with severe or atypical GERD symptoms, when other diseases may be present, or when a treatment trial with a PPI is ineffective.15 Endoscopy is useful for diagnosing complications of GERD, such as Barrett’s esophagus, esophagitis, and strictures. Fewer than 50% of patients with GERD symptoms have evidence of esophagitis on endoscopy.16
The American Society for Gastrointestinal Endoscopy recommends endoscopy when there are clinical suggestions of severe reflux or other disease.17 The American College of Gastroenterology recommends further testing
when empiric therapy has failed
when symptoms of complicated disease exist
when there is dysphagia, bleeding, weight loss, choking, chest pain, or long-standing symptoms
The Canadian Consensus Conference recommends endoscopy in the presence of
dysphagia
odynophagia
bleeding
weight loss
noncardiac chest pain
failure to respond to 4 to 8 weeks of pharmacologic therapy.19
It also recommends a single test if maintenance therapy is required.
Other diagnostic tests
Other diagnostic tools may be of use in some settings.
A barium esophagram can document reflux, and Bernstein testing (esophageal acid infusion test) can identify esophageal hypersensitivity to acid, although neither establishes a diagnosis of GERD. Ambulatory 24-hour intraesophageal pH monitoring can help to establish the presence of GERD by documenting the proportion of time during which the intraesophageal pH is acidic (<4) and can also establish the degree of association between patients’ symptoms and episodes of esophageal acidification.
Esophageal manometry is not recommended as a routine diagnostic test for GERD. It is important in selected patients to exclude an esophageal motility disorder and may be necessary as part of the pre-operative evaluation for patients in whom a surgical operation for GERD is being considered.
Management of gerd
GERD commonly requires long-term management that includes dietary, lifestyle, and pharmacological interventions. Surgery may be considered for the long-term management of the condition in carefully selected patients.