Diagnosis: Secondary syphilis
Our patient’s “moth-eaten” alopecia—an uncommon sign of syphilis—heightened our suspicion of this sexually transmitted infection and prompted us to ask additional questions about his sexual history. We learned that our patient had engaged in unprotected sex with a male partner approximately 6 months prior to his unusual hair loss. Shortly after that encounter, the patient went to his primary care physician for screening of sexually transmitted diseases after his partner had complained of a new lesion on his penis. At that screening, our patient was tested for chlamydia, gonorrhea, herpes simplex virus (HSV), and human immunodeficiency virus (HIV), and was given a rapid plasma reagin (RPR) test. He was positive only for HSV-1.
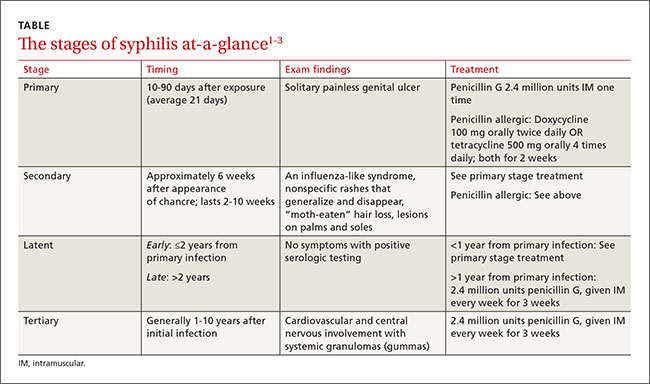
How “the great imitator” presents. A solitary painless genital ulcer marks the first (primary) stage of infection with the spirochete Treponema pallidum (TABLE1-3). Secondary syphilis results from the hematogenous or lymphatic spread of the Treponema pallidum spirochete, and often results in dermatologic findings that mimic numerous other conditions. Patients may also experience fever and myalgia. Typically, secondary syphilis lesions are pink and scaly 1 to 2 cm patches, which generalize in 80% of patients.2 Alopecia in a “moth-eaten” pattern is an uncommon finding of secondary syphilis, and should prompt a thorough sexual history.