William D. Anderson, III, MD, DABFM, FAAFP Nathaniel S. Treister, DMD, DMSc E.J. Mayeaux, Jr., MD, DABFM, FAAFP Romesh P. Nalliah, DMD University of South Carolina School of Medicine, Columbia (Drs. Anderson and Mayeaux); Brigham and Women’s Hospital, Boston (Dr. Treister); Harvard Medical School, Boston (Dr. Nalliah) william.anderson@uscmed.sc.edu
The authors reported no potential conflict of interest relevant to this article.
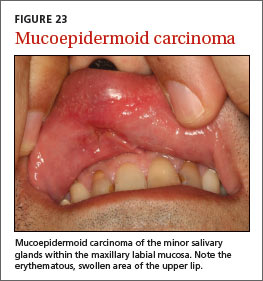
Non-SCC cancers. Salivary gland tumors are rare and most commonly occur in patients ages 55 to 65 years. Most neoplasms (70%-85%) occur in the parotid gland, while 8% to 15% develop in the submandibular salivary gland and less than 1% involve the sublingual gland.21 Minor salivary gland tissue, especially in the lips and palate, may also be affected (FIGURE 23). Patients present with circumscribed, fixed or movable, painless, soft or firm masses in a salivary gland.
Melanoma should be included in the differential diagnosis of oral pigmented lesions that have any features of cutaneous melanoma, such as asymmetry, irregular borders, or variable or changing color.22
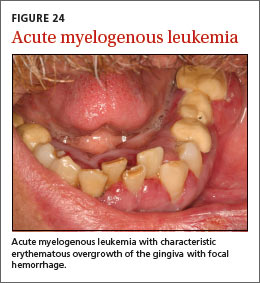
Hematologic malignancies may initially present (or demonstrate evidence of relapse) in the oral cavity. Leukemia typically presents with sheet-like overgrowth and swelling of the gingiva with associated erythema and bleeding (FIGURE 24), whereas lymphoma typically presents as a solitary mass or ulceration. Solid tumors that metastasize to the oral cavity may present with localized unexplained soft or hard tissue growths, with or without associated neurologic symptoms (eg, paresthesia).
CORRESPONDENCE William D. Anderson, III, MD, DABFM, FAAFP, University of South Carolina School of Medicine, 15 Medical Park, Suite 300, Columbia, SC 29203; william.anderson@uscmed.sc.edu