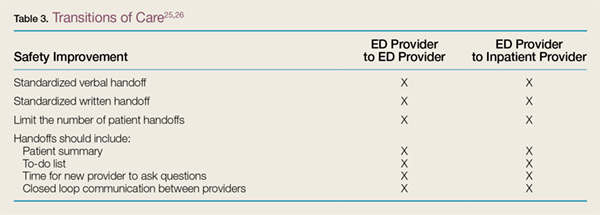
Many ED patients will need transition from “ED patient” to “admitted patient”—ie, admission to the hospital and transfer of care to an inpatient service provider. Studies on transitions of care from the ED to an inpatient medical service have found multiple barriers to a seamless transition of care. These include communication failures; information technology failures; inability of inpatient providers to review vital signs, laboratory values, and medications given; a change of the inpatient team to whom the patient was assigned; and patient transfers to areas remote from the ED and/or inpatient floors, such as to a dialysis unit. In one survey, 29% of respondents reported that a patient of theirs had experienced an adverse event or near misses due to a poor handoff between the ED and medical service.26 Just as there needs to be a standardized process for ED-provider-to-ED-provider handoffs, there also should be a standardized process for ED-to-inpatient or -outpatient service provider handoffs. There should be verbal and possibly written transmission of vital information, with patient summaries, “to-do” lists of follow-ups, situational knowledge with contingency planning, and time for questions (Table 3).25,26 The Joint Commission’s Transitions of Care Portal (https://www.jointcommission.org
/toc.aspx) offers tools to help facilities formalize this process.
Health Information Technology
Case Scenario 4
An EM intern was instructed to order a dose of morphine for a patient with a fractured hip. The intern used electronic ordering. Afterward, the nurse caring for the patient asked the attending EP if she really wanted to order patient-controlled morphine analgesia for the patient. Upon reviewing the order, the attending discovered the intern had selected the first morphine on the drop-down list instead of scrolling down to find the range of individual doses available.
Discussion
The use of electronic health records (EHRs) and health information technology (HIT) systems has both improved patient care and introduced new errors. Physician handwriting may no longer be a problem, but some hospitals use several types of EHRs simultaneously, with different systems for inpatients, outpatients, and EDs. In these settings, there may not be a seamless system to allow for review of inpatient, outpatient, and ED records. Additional concerns include communication failure, misidentification of patient orders, poor data display, and “alert fatigue.”27 Communication failures include the lack of bedside or face-to-face discussion among care providers. Physicians may enter orders at a computer away from the nursing station and never directly inform the nurse about the plan for the patient.
Incorrect patient orders are usually self-explanatory. Other errors include choosing the wrong LASA medication from a drop-down list or ordering imaging studies for the wrong side of the patient’s body. Poor data display may not alert providers of two or more patients with the same last name or allow vital signs to be displayed in a meaningful way. Other data-display problems include the inability to distinguish abnormal results from normal results because the system uses the same display color for both. Conversely, alert fatigue occurs when too many warning messages appear while providers are trying to enter orders for patient care. These warnings can range from important messages such as allergy identification or severe drug interactions to noncritical alerts about the cost of a test.
Recommendations to improve patient safety with the use of EHRs or HIT systems involve having a frontline staff champion to identify areas for performance improvement and having a review process to identify and examine safety issues with these technologies. A multidisciplinary group, including frontline staff, can usually develop effective solutions to these safety issues.27
Conclusion
The ED is a high-risk setting for errors because it features high-acuity patients, patients of widely divergent ages, the frequent need to use high-alert medications, the need to simultaneously care for multiple patients, many interruptions and distractions, and the lack of an established relationship with patients. This environment can lead to communication failures in handoffs and transitions of care, medication errors, and poor follow-up due to poor discharge processes. Additional difficulties arise when HIT systems, such as EHRs, are not set up to ensure the success of frontline staff caring for ill patients. The ED can become a much safer place by establishing strategies such as those outlined in this article to reduce error in all of these areas.