By Mary Ann Moon
From JAMA

These findings—from an analysis of two large nationally representative data sets—paint a picture that is complex and more nuanced than that suggested by some recent reports. For example, a study of the Researched Abuse, Diversion, and Addiction-Related Surveillance (RADARS) System found that the abuse and diversion of prescription opioids plateaued or decreased in recent years.3 “The nationally representative results in our study may be especially important in providing an accurate picture of the current status of the epidemic,” said Dr Beth Han of the Substance Abuse and Mental Health Services Administration (SAMHSA), Rockville, Maryland, and her associates.
The nonmedical use of prescription opioids is an acknowledged epidemic, but that epidemic’s changing pattern over time needed to be updated. The investigators assessed the changes in use during the most recent decade for which data are available (2003-2013) using annual surveys conducted by SAMHSA and cause of death files from the National Vital Statistics System.
Based on responses from 472,200 people aged 18 to 64 years, the 1-year prevalence of nonmedical use of prescription opioids decreased from 5.4% to 4.9% during the study period. However, the 1-year prevalence of use disorders rose from 0.6% to 0.9%, the 1-year prevalence of high-frequency use (200 days or more per year) increased from 0.3% to 0.4%, and the rate of opioid-related deaths increased from 4.5 per 100,000 to 7.8 per 100,000. In addition, the mean number of days of opioid abuse increased from 2.1 to 2.6 per year in the general population and from 40.0 to 54.2 days per year among acknowledged opioid users, the investigators said.1
Compared with white users of prescription opioids, both black and Hispanic users had a lower prevalence of use disorders. The prevalence of use disorders was higher among less-educated than more-educated adults, among those with no health insurance or Medicaid as opposed to private health insurance, and among smokers than nonsmokers, Dr Han and her associates added.
Previous research has shown that most adults who abuse prescription opioids neither receive treatment nor perceive that they need treatment. Clinicians can help by using prescription-drug monitoring programs to identify inappropriate receipt of prescription opioids, then offering treatments, which are highly effective, for patients who need them, the investigators noted.
Views on the News
Keep Patients Opiate Naive
The slight decline (approximately 0.4% over 10 years) in opioid initiation reported by Han et al1 may be encouraging, but their other findings suggest that more patients are experiencing an inexorable progression from initial opioid use to frequent use to highly frequent use to a use disorder.
The source of most opioid abuse is often a seemingly legitimate prescription, and the key to addressing the opioid-abuse epidemic is to keep opioid-naive patients opioid naive. It is still unclear why clinicians continue to prescribe opioids, despite recommendations to the contrary and the fact that these agents provide little or no long-term benefit for most types of chronic pain.
Lewis S. Nelson, MD, is in the Ronald O. Perelman department of emergency medicine at New York University. He and his associates made these remarks in an editorial2 accompanying Dr Han’s report.1
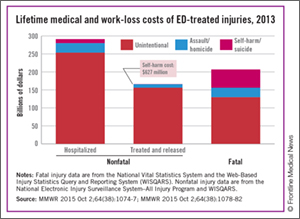
US Injury Costs Topped $671 Billion in 2013
By Richard Franki
From MMWR
Over 30 million injuries were treated in US EDs in 2013, costing an estimated $671 billion, the CDC reported.
The largest share of that cost—almost $290 billion, or about 43%—came from the 3 million persons with nonfatal injuries who were hospitalized. Costs for the 27 million people who were treated and released from EDs were $167 billion, which was just under 25% of the total. The lifetime cost estimate for the almost 193,000 injury-associated deaths in 2013 was over $214 billion (32%), said Curtis Florence, PhD, of the CDC’s National Center for Injury Prevention and Control, Atlanta, Georgia, and associates.
For each ED-treated injury-related death, the mean cost in terms of lost lifetime earnings and medical care provided was just over $1.1 million: Homicides cost over $1.6 million, suicides were $1.2 million each, and each unintentional injury death cost just under $1 million, they said.1
Drug poisonings, including prescription drug overdoses, accounted for the largest share of fatal injury costs (27%), followed by transportation-related deaths (23%) and firearm-related deaths (22%), Dr Florence and associates noted.