To the Editor:
Syringoma is a relatively common benign adnexal neoplasm originating in the ducts of eccrine sweat glands. It can be divided into 4 variants based on clinical features: localized; familial; Down syndrome associated; and generalized, which includes multiple syringomas and eruptive syringoma (ES).1 Eruptive syringoma is a rare variant of generalized syringoma that was first described by Jacquet and Darier2 in 1887. Clinically, ES lesions manifest as multiple nonfused, flesh-colored to reddish-brown papules that are located most commonly on the anterior trunk during childhood or adolescence. Eruptive syringoma can be missed easily or misdiagnosed clinically. We present 3 rare cases of ES.
A 28-year-old man presented with multiple asymptomatic papules on the trunk and upper arms of 20 years’ duration (patient 1). He had been diagnosed with Darier disease 3 years prior to the current presentation and was treated with oral and topical retinoic acid without a response. After 3 months of oral treatment, the retinoic acid was stopped due to elevated liver enzymes. Physical examination at the current presentation revealed multiple smooth, firm, nonfused, 1- to 4-mm, reddish to dark red papules on the neck, chest, abdomen, and flexural surfaces of the upper arms (Figure 1A). Dermoscopy of the arm lesions showed light brown pigment networks and yellowish-white unstructured areas surrounded by linear vessels on a pink background under polarized light (Figure 1B). Histopathologic examination of a lesion on the left arm revealed epithelial cords, ducts, and cystic structures within the superficial and mid dermis. The ducts were lined by 2 rows of epithelial cells with a characteristic tadpolelike pattern and filled with eosinophilic amorphous substances (Figure 1C).
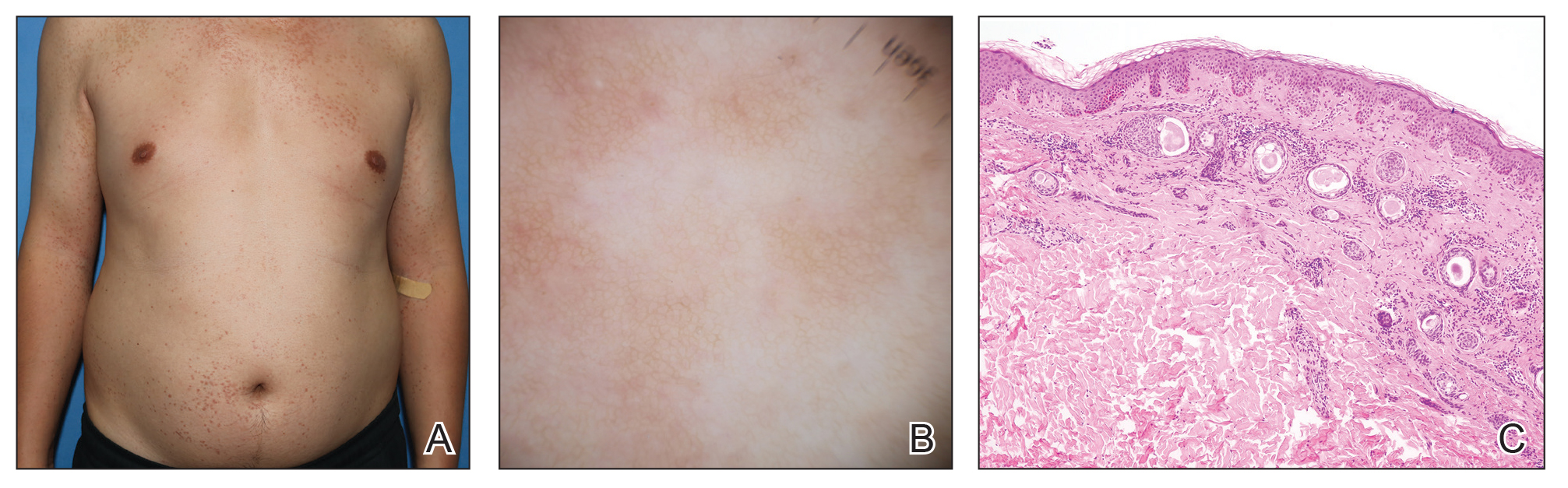
FIGURE 1. A, Multiple smooth, firm, nonfused, 1- to 4-mm, reddish to dark red papules on the chest, abdomen, and flexural surfaces of the arms in a patient with eruptive syringoma. B, Dermoscopy of the arm lesions showed light brown pigment networks and yellowish-white unstructured areas surrounded by linear vessels on a pink background. C, Histopathologic examination of a left arm lesion showed some ducts with a tadpolelike pattern in the dermis (H&E, original magnification ×100).
A 27-year-old woman presented with widespread asymptomatic papules of 8 years’ duration (patient 2). She denied any use of drugs. Physical examination revealed multiple flesh-colored to reddish papules on the face, armpits, trunk, thighs, and vulva (Figure 2).

FIGURE 2. Eruptive syringoma consisting of multiple flesh-colored to reddish papules on the vulva.
A 43-year-old man who was otherwise healthy presented with brownish flat-topped papules on the chest and abdomen of 19 years’ duration (Figure 3A)(patient 3). The lesions had remained stable and did not progress. He denied any treatment. Dermoscopy of the chest lesions showed a light brown pigment network as well as dotted and linear vessels on a pale yellow background (Figure 3B).
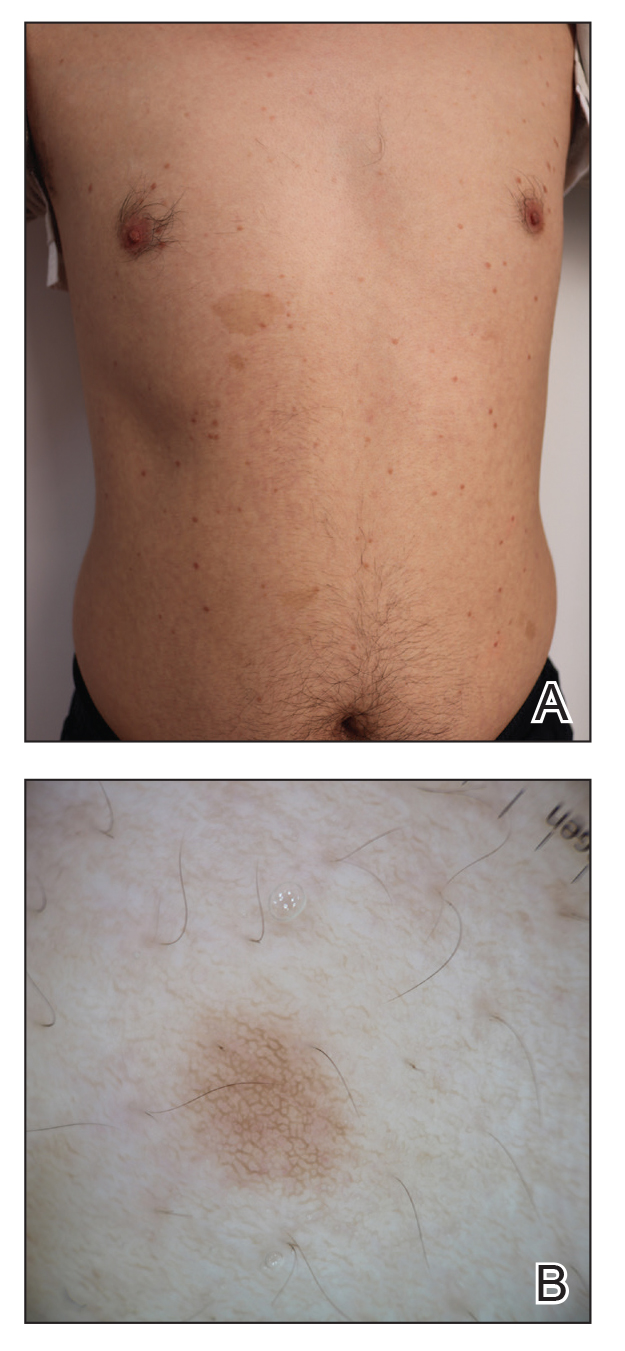
FIGURE 3. A, Multiple brownish flat-topped papules on the trunk in a patient with eruptive syringoma. B, Dermoscopy of the chest lesions showed a light brown pigment network as well as dotted and linear vessels on a pale yellow background.
All 3 patients demonstrated classic histopathologic features of syringoma, and none had a family history of similar skin lesions. The clinical and dermoscopic findings along with the histopathology in all 3 patients were consistent with ES. In patient 1, three sessions of electrocautery treatments on both upper arms were performed with settings of short-fire mode (1–3 V) at 4- to 8-week intervals. After treatment, the lesions subsided but recurred 7 months later. Five months after recurrence, the rash gradually increased on the trunk and upper arms. In patient 2, two sessions of CO2 laser treatments on the trunk were performed with settings of modulated pulse mode (1–2 W) at 4- to 8-week intervals. The lesions disappeared after treatment but recurred 6 months later. At 1-year follow-up after recurrence, the rash had increased slightly. Neither patient 1 nor patient 2 developed hyperpigmentation or scarring during the 1-year follow-up period after their respective treatments. Patient 3 opted not to undergo treatment after being informed that the lesions were benign, and his condition stabilized at 1-year follow-up.
The pathogenesis of ES is unclear, but it may be affected by hormones, autoimmune status, immunosuppression (eg, liver and kidney transplantation), and medications (eg, hypersensitivity, phototoxicity, and antiepileptic medications).3-6 Guitart et al7 hypothesized that ES may be a hyperplastic response of the eccrine duct to an inflammatory reaction, such as trauma from waxing or chronic scratching. It also has been associated with systemic conditions such as Nicolau-Balus syndrome (syringomas, milia, and atrophoderma vermiculata) and Down syndrome.8,9 The lesions manifest symmetrically and are characterized by flesh-colored to reddish-brown, shiny, or flat-topped papules; however, ES also can manifest as hyperpigmentation, erythema, positive Darier sign, or pseudokoebnerization.10 The lesions typically are located on the eyelids, neck, anterior chest, upper abdomen, upper arms, axillae, and genital region, and they rarely involve the palms, soles, and mucous membranes. Eruptive syringoma commonly is asymptomatic and in rare cases gradually subsides.11
Sometimes the lesions of ES are atypical and clinically resemble Darier disease, Fox-Fordyce disease, lichen planus, mastocytosis, granuloma annulare, trichoepithelioma, and sarcoidosis. Additionally, Marfan syndrome and Ehlers-Danlos syndrome should be ruled out when lesions involve the eyelids.11 The differential diagnosis in our patients included Darier disease and Fox-Fordyce disease, which can be differentiated from ES via noninvasive dermoscopy and pathologic biopsy. In most patients with ES, dermoscopic findings include reticular brown lines or fine pigment networks as well as dotted and linear or reticular vessels. Tiny whitish dots, multifocal hypopigmented areas, and glittering yellow-whitish round structures are dermoscopic hallmarks of the vulvar variant of ES.12-14 Histopathology of ES has shown epithelial cords, ducts, and cystic structures within the dermis. The ducts are lined by 2 rows of epithelial cells with a characteristic comma-shaped/tadpolelike pattern and are filled with eosinophilic amorphous substances. The dermoscopic features of Darier disease differ from ES in that Darier disease usually manifests as a comedolike opening with a central polygonal yellowish-brownish structure surrounded by a whitish halo on a pink background.15 Histopathology of Darier disease has shown acantholysis above the basal layer of the epidermis and dyskeratotic keratinocytes. Dermoscopic findings in Fox-Fordyce disease include typical light brown to dark brown, folliculocentric, structureless areas with loss of dermatoglyphics. Some of the lesions also show hyperkeratotic follicular plugging.16 Histopathology of Fox-Fordyce disease includes infundibulum dilation, hyperkeratosis, plugging, acanthosis, a lymphohistiocytic infiltrate, and a perifollicular foam cell infiltrate.17Eruptive syringoma is a benign condition that generally requires no treatment. The goal of treatment is to improve cosmesis and primarily includes physical and chemical therapies such as surgical resection, cryosurgery, electrodesiccation, CO2 laser (alone and in combination with trichloroacetic acid10), argon laser, fractional photothermolysis, dermabrasion, and chemical peeling. However, because ES involves deeper areas of the dermis, some treatments may cause hyperpigmentation, scar formation, or recurrence of the lesions and may be less effective for lesions on the eyelids, which may remain untreated. Systemic therapy consists of oral retinoic acid or tranilast.18 The use of topical retinoic acid and atropine also have been reported,19 but their efficacy remains uncertain. The lesions in patient 1 did not resolve after receiving oral and topical retinoic acid. Although ES lesions may decrease in size or subside without intervention in rare cases, the disease was not self-limiting in our patients.