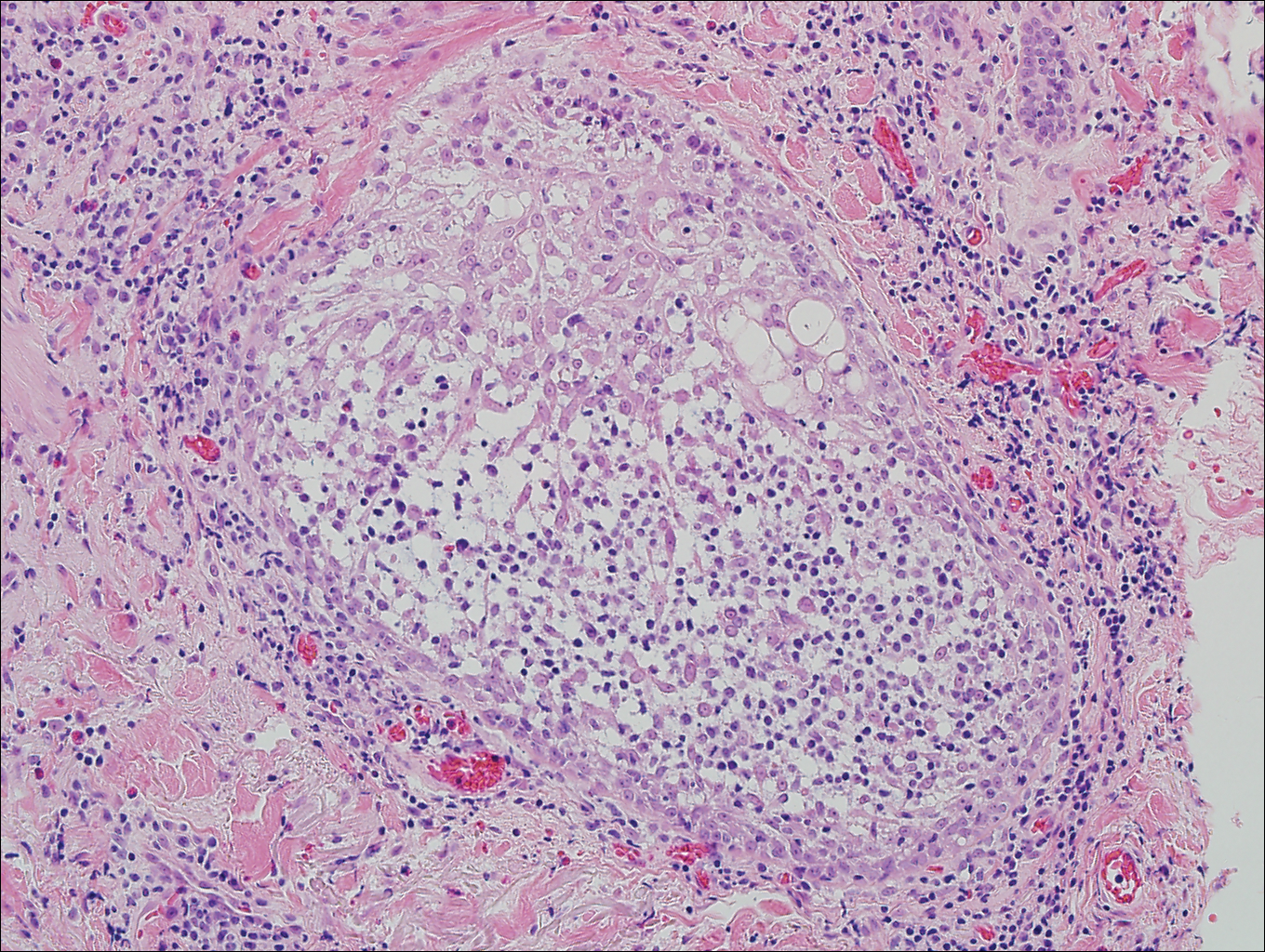
Primary follicular mucinosis (PFM) tends to occur as a solitary lesion in younger female patients in contrast to the multiple lesions that typically appear in older male patients with FMF. Histologically, PFM usually manifests as large, cystic, mucin-filled spaces and polyclonal perivascular and periadnexal lymphocytic infiltrate without notable cellular atypia or epidermotropism (Figure 3). Because follicular mucinosis is a common feature of FMF, its distinction from PFM can be challenging and often is aided by the absence of cellular atypia and relatively mild lymphocytic infiltrate in the latter.7
 Photograph courtesy of Brian Swick, MD (Iowa City, Iowa).
Photograph courtesy of Brian Swick, MD (Iowa City, Iowa).
Figure 3. Follicular mucinosis with mucin-filled cystic spaces (H&E, original magnification ×4).
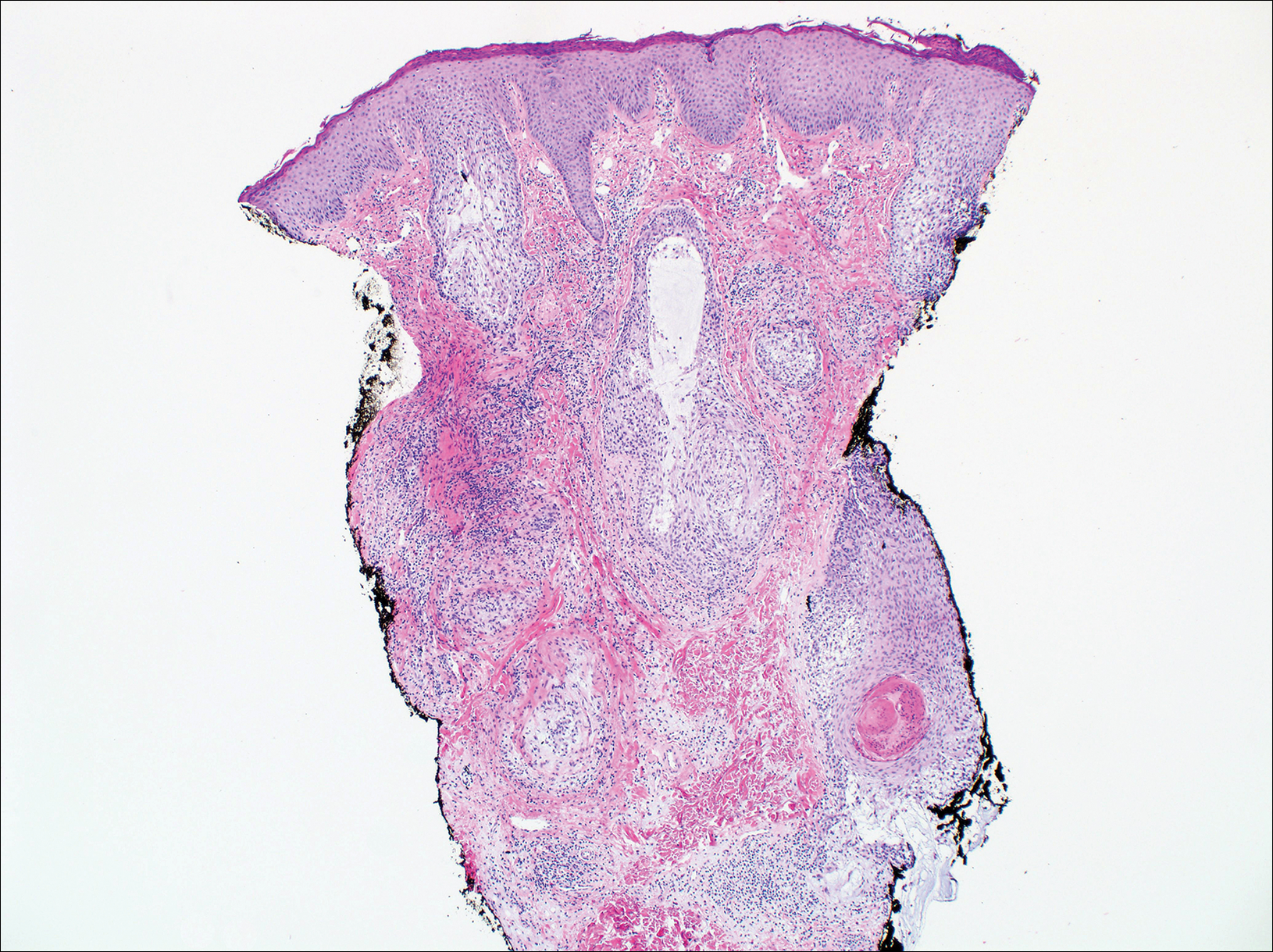
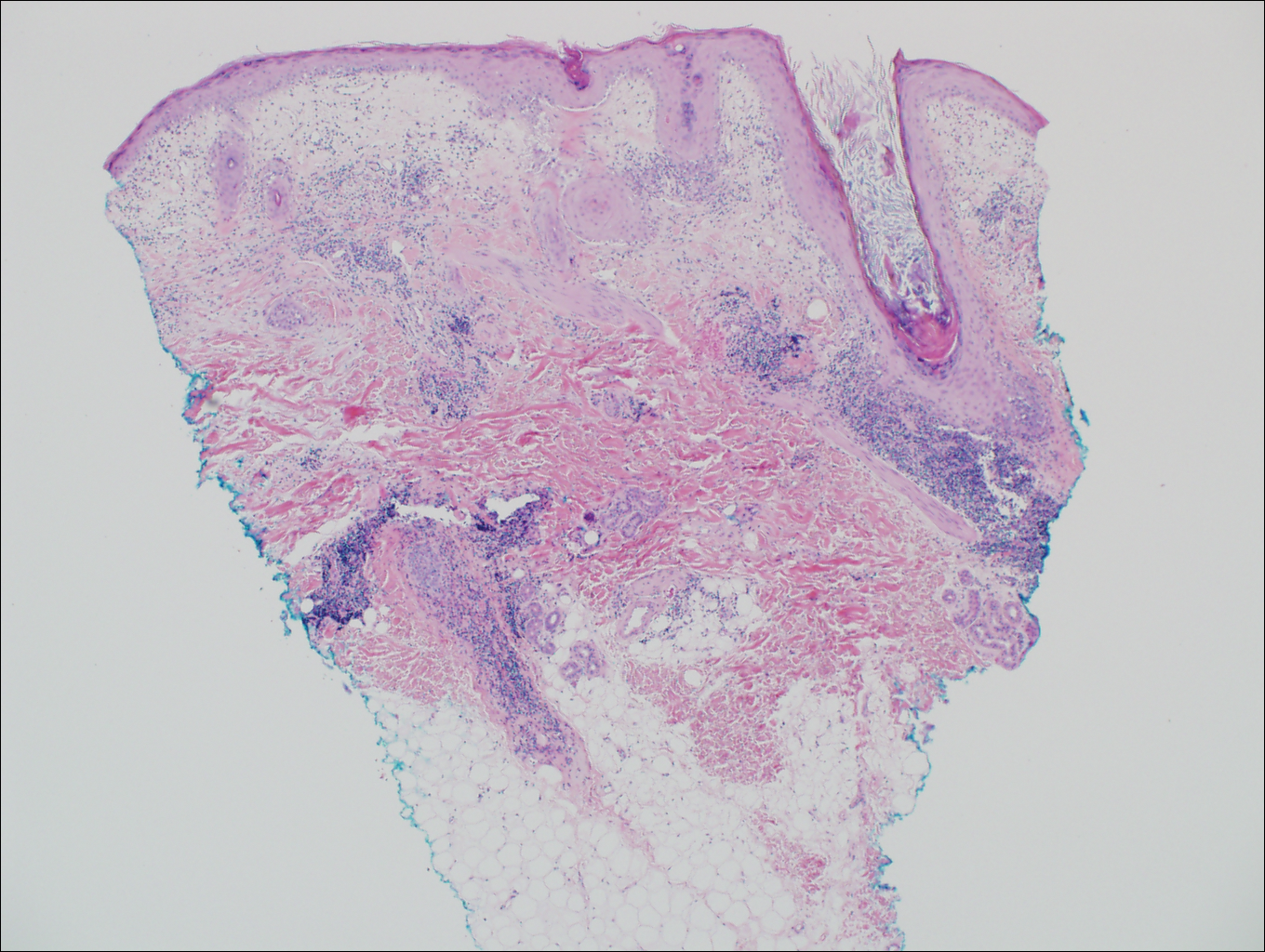
Cutaneous lupus erythematosus with its characteristic folliculocentric lymphocytic infiltration and associated dermal mucin also qualifies as a potential differential possibility for FMF; however, the perivascular and periadnexal pattern of lymphocytic infiltration as well as the localization of mucin to the reticular dermal interstitium8,9 are key histopathologic distinctions (Figure 4). Furthermore, although the histologic presentation of lupus erythematosus can be variable, it also classically shows interface dermatitis, basement membrane thickening, and follicular plugging.
 Photograph courtesy of Brian Swick, MD (Iowa City, Iowa).
Photograph courtesy of Brian Swick, MD (Iowa City, Iowa).
Figure 4. Cutaneous lupus erythematosus with interface dermatitis as well as a perivascular and periadnexal lymphocytic infiltrate with follicular plugging (H&E, original magnification ×4).
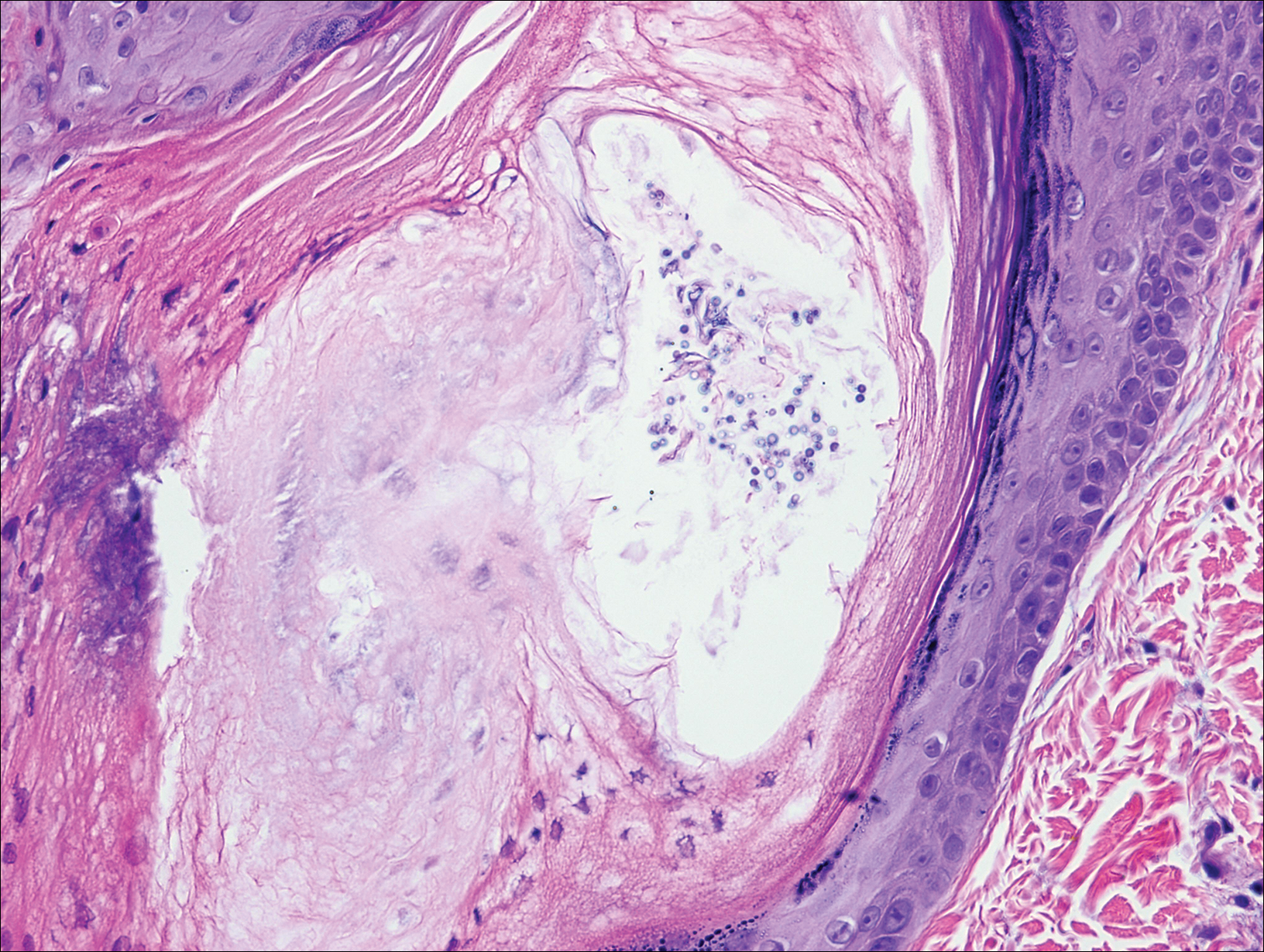
Pityrosporum folliculitis is the most common cause of fungal folliculitis and is caused by the Malassezia species. On histology, there typically is an unremarkable epithelium with plugged follicles and suppurative folliculitis. Serial sections of the biopsy specimen often are required to identify dilated, follicle-containing, budding yeast cells (Figure 5). Organisms are located predominantly within the infundibulum and orifice of follicular lumen, are positive for periodic acid-Schiff, and are diastase resistant.10
 Photograph courtesy of Brian Swick, MD (Iowa City, Iowa).
Photograph courtesy of Brian Swick, MD (Iowa City, Iowa).
Figure 5. Pityrosporum folliculitis with budding yeast forms (H&E, original magnification ×40).