Interpreting the results: The experts disagree
The ADA recommends that patients with diabetes and hypertension be treated to a goal <140 mm Hg systolic and <80 mm Hg diastolic pressure11—more lenient than the recommendations of either the AACE or the IDF. It is not clear whether these recommendations will change, however, given the recent JNC 8 report.1 A lower systolic target may be appropriate for certain patients, if it can be achieved without undue adverse effects from antihypertensive medication. Older patients in particular may be at risk for orthostasis or falls as a result of more aggressive treatment.
CASE › Mr. D’s most recent BP is 145/95. Given that his goal is <140/90, you elect to start lisinopril 10 mg daily, advise him to monitor his BP at home, and refer him to a dietician to discuss the Dietary Approaches to Stop Hypertension diet.
Lipid levels: When to add statin therapy
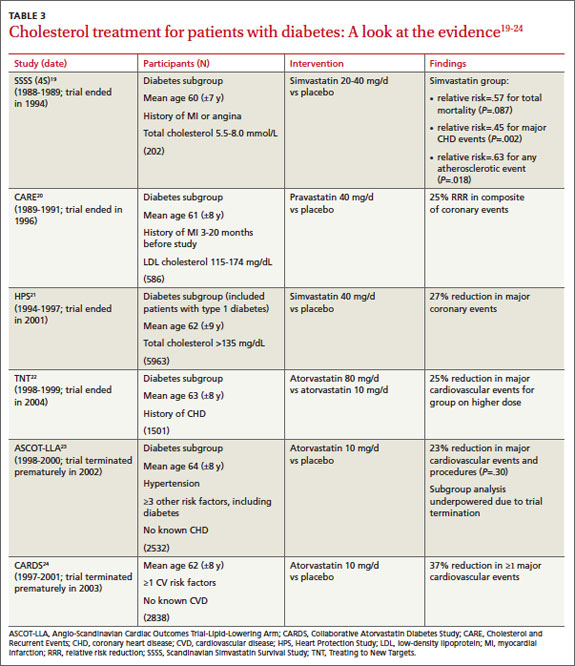
Like glucose and BP control, lipid control and, concomitantly, the benefit of statin therapy for patients with type 2 diabetes has been studied extensively (TABLE 3).19-24
The Scandinavian Simvastatin Survival Study (4S) recruited participants with a history of MI or angina, and included a small diabetes subgroup.19 Participants were randomized to simvastatin 20 mg daily, with blinded titration up to 40 mg/d, or placebo. Among those with diabetes, patients on simvastatin had a 55% reduction in risk for major coronary heart disease events and a 43% reduction in total mortality. The risk reduction did not depend on baseline levels of total cholesterol, LDL cholesterol, HDL cholesterol, or triglycerides.
Cholesterol and Recurrent Events (CARE), which studied participants with a history of MI 3 to 20 months prior to the start of the study and also included a diabetes subgroup, had a similar outcome.20 Compared with placebo, treatment with pravastatin 40 mg/d reduced the risk of both coronary events and revascularization procedures by 25%.
The Heart Protection Study randomized patients with either diabetes or a history of occlusive arterial disease to receive simvastatin 40 mg daily or placebo.21 In the treatment group, the risk of major vascular events was reduced in patients with diabetes by 27%. Improvements were seen in patients with LDL cholesterol levels both above and below 116 mg/dL.
Multiple studies have evaluated the benefits of atorvastatin for patients with diabetes. All have demonstrated a significant reduction in the risk of MI and death in those on statin therapy. The Treating to New Targets study showed a 25% reduction in major cardiovascular events in those treated with 80 mg atorvastatin daily (mean LDL, 77 mg/dL) vs those treated with 10 mg of the drug (mean LDL, 86 mg/dL).22 The Anglo-Scandinavian Cardiac Outcomes Trial–Lipid-Lowering Arm (ASCOT-LLA)23 and the Collaborative Atorvastatin Diabetes Study (CARDS)24 were both terminated early due to the magnitude of benefit seen with statin therapy. In contrast to LDL, evidence for non-LDL treatment goals is lacking in the diabetes literature. Also, there is little evidence to support nonstatin cholesterol-lowering therapy for the management of diabetes patients.
Continue for statin use >>