Autonomous advanced practice clinicians in high-risk practice settings have an immense responsibility to ensure that their patients are getting the best possible care. It is documented that as expertise develops, knowledge and decision processes change. Ordinarily, highly experienced clinicians use the more time-efficient System 1 process when faced with common disorders; for more complex disorders, they change to System 2 thinking to facilitate a more comprehensive evaluation.13 In many instances, however, a provider may inadvertently take shortcuts to conclude the clinical encounter, including relying on intuitive thinking—which can be prone to bias—when analytic thinking is necessary.
Clinicians are usually unaware of the influence that biases may have on their decision making and should reflect on their behavior to determine if any biases exist. To improve patient safety and facilitate better care, all providers should perform a personal inventory to identify CDRs they may have developed. Questions that will help to reveal CDRs include
- Am I rushing to get off my shift on time?
- Was the patient “turned over” to me at the shift change?
- Have I allowed a previously negative experience with this patient to influence my objectivity and clinical decision-making?
- Am I tired?
- Has the diagnosis been suggested by the nurse, paramedic, or the patient’s family?9
- Has the diagnosis been suggested by the nurse,
If one or more biases are found, a purposeful effort to mentally “uncouple” from a bias should be done. This process is referred to as metacognition, or thinking about one’s own thought processes.9 Paramount among the thinking processes that may be at play is an awareness of how System 1 and System 2 thinking interact and affect clinical decision making, as this enables the clinician to recognize which mode of thinking they use to arrive at a decision and when they need to shift from intuitive to analytic thinking.
Another factor to consider is overconfidence: Berner and Graber note that a provider’s overconfidence3 in his or her own knowledge and experience and lack of awareness of when an “override” is needed can be a cause of diagnostic errors.18 The tendency to shore up existing beliefs rather than force a new cognitive strategy is a sign of a rigid thinking process that may ultimately result in a poor clinical decision.9 Finally, providers should be aware of their surroundings and practice environments. As noted earlier, emergency medicine, family medicine, internal medicine, and urgent care have high diagnostic error rates due, in part, to high patient volumes.1
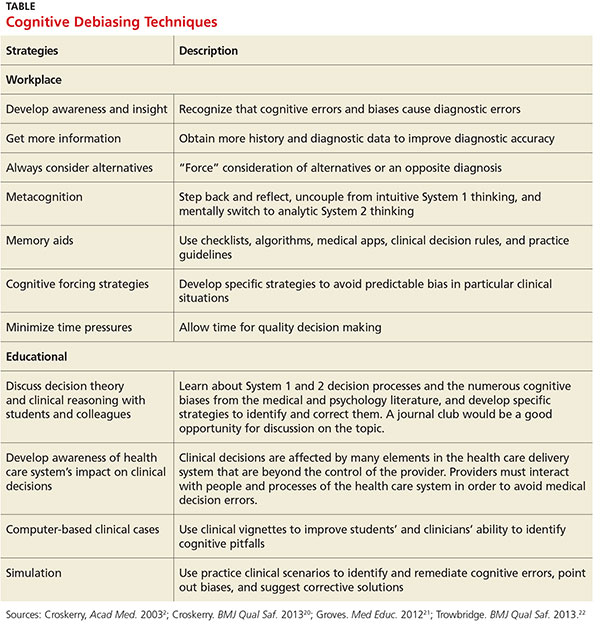
Once a tendency for a certain cognitive bias is recognized, the next step is to develop a sustainable method to counteract it, a process referred to as debiasing, to prevent cognitive errors. The table lists some workplace and educational debiasing techniques that have been described in the literature.20,21 Critics of cognitive debiasing argue that CDRs are preconscious, that awareness of CDRs is not enough to counteract their effects, and that there is no ability for one to develop “generic” conscious efforts to counter them.14 Their concern here is that a clinician may be able to counter a bias in one clinical context but not in another.14 It is clear that clinical reasoning is complex and involves many interrelated elements, such as clinical knowledge and critical thinking, with System 1 and 2 thinking working in tandem and metacognition overarching the whole process.21 Errors in diagnosis can have multiple causes and no single cognitive approach can be effective in addressing all of these causes. Knowing about cognitive bias helps clinicians address one possible element underlying diagnostic errors. Efforts to eliminate bias in clinical reasoning should begin early in clinical education; this can be done by incorporating instruction on clinical reasoning, including the relationship between intuitive and analytic decisions, metacognition, and awareness of the strengths and weaknesses of heuristics.22
In summary, in clinical situations where bias or uncertainty might exist, a clinician can make an effort to avoid a bad decision by
- Stepping back and reflecting to consider if a bias exists.
- Developing rules and mental procedures to reject a reflexive automatic response and force a “System 2 override.”9
- Developing “mental-ware” (mental techniques) to uncouple from a recognized or recurring cognitive bias.9
Continue to conclusion >>